Wolff-Parkinson-White (WPW) Syndrome: Causes, ECG Features, Symptoms, Diagnosis, and Treatment.
Wolff–Parkinson–White (WPW) syndrome is a congenital heart rhythm disorder caused by an extra electrical pathway between the atria and ventricles. This article explains the causes, ECG findings, symptoms, diagnosis, complications, and treatment options of WPW syndrome in a clear, patient-friendly way, with special focus on critical care awareness and nursing education.
Educational Content Only
This article is written for educational purposes and does not constitute medical advice. Always consult a qualified healthcare professional before making clinical or personal health decisions. Read our disclaimer.
Introduction
Wolff-Parkinson-White (WPW) syndrome is a congenital cardiac conduction disorder caused by an abnormal extra electrical pathway between the atria and ventricles of the heart. This pathway is commonly called an accessory pathway or the Bundle of Kent.
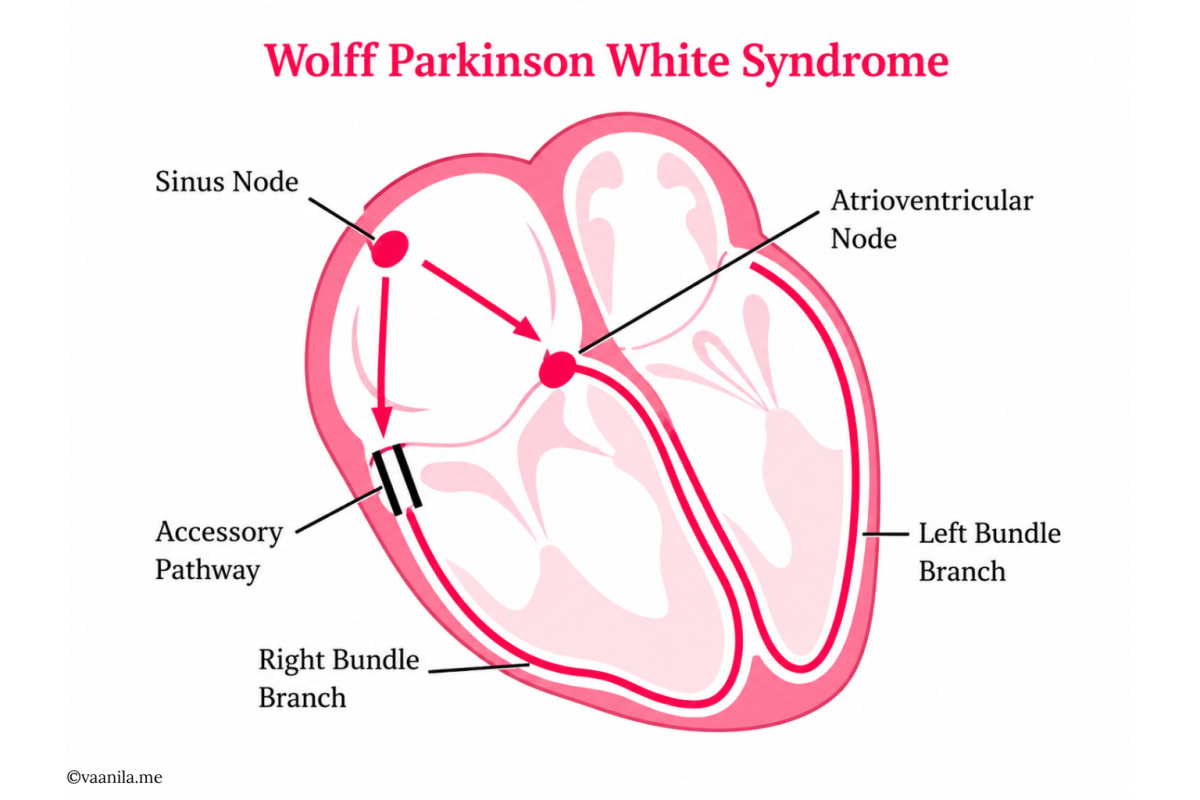
In a normal heartbeat, electrical impulses pass from the atria to the ventricles through the atrioventricular node (AV node), where there is a brief delay. In WPW, the accessory pathway allows some impulses to bypass this normal AV nodal delay and reach the ventricles too early. This early ventricular activation is known as ventricular pre-excitation.
WPW is relatively uncommon, affecting approximately 1 to 3 people per 1,000. Some individuals have no symptoms and are diagnosed only after an electrocardiogram (ECG), while others experience episodes of palpitations, rapid heartbeat, dizziness, chest discomfort, shortness of breath, or fainting.
History
WPW syndrome was first described in 1930 by Louis Wolff, John Parkinson, and Paul Dudley White. They reported patients with episodes of rapid heartbeat, a short PR interval, a widened QRS complex, and no obvious structural heart disease. The condition was later named Wolff-Parkinson-White syndrome in recognition of these physicians.
Definition
Wolff-Parkinson-White syndrome is a pre-excitation syndrome caused by an abnormal accessory conduction pathway between the atria and ventricles. This pathway produces characteristic ECG changes and can predispose the patient to tachyarrhythmias.
In simple words, WPW means the heart has an extra electrical shortcut. This shortcut can activate the ventricles earlier than normal and may sometimes trigger sudden fast heart rhythms.
WPW Pattern vs. WPW Syndrome
This distinction is clinically important. WPW pattern refers to characteristic ECG changes without symptoms. WPW syndrome refers to the presence of ECG changes together with symptoms such as palpitations, tachycardia, dizziness, or syncope.
Therefore, WPW pattern is an ECG finding, while WPW syndrome includes both ECG findings and clinical manifestations.
Normal Cardiac Conduction
Normally, the heartbeat begins in the sinoatrial node (SA node), the natural pacemaker of the heart. The electrical impulse travels from the SA node through the atria, reaches the AV node, then passes through the Bundle of His, the right and left bundle branches, the Purkinje fibers, and finally the ventricles.
The SA node initiates the heartbeat and helps regulate heart rate. The AV node acts as a natural delay point, briefly slowing the impulse before it enters the ventricles. This delay allows the ventricles to fill with blood before contraction.
Pathophysiology of WPW Syndrome
In WPW syndrome, an accessory pathway connects the atria and ventricles outside the usual AV nodal route. Because the accessory pathway does not slow conduction in the same way as the AV node, electrical signals can reach the ventricles earlier than expected.
This abnormal conduction produces three key effects: ventricular pre-excitation, a delta wave on ECG, and the possibility of a re-entry circuit.
Key Mechanisms
Ventricular pre-excitation: part of the ventricle is activated earlier than usual.
Delta wave: the beginning of the QRS complex appears slurred because ventricular activation starts through ordinary heart muscle before the normal His-Purkinje system completes conduction.
Re-entry circuit: electrical impulses may travel in a circular loop using both the normal AV nodal pathway and the accessory pathway. This can cause sudden episodes of rapid heartbeat, most commonly atrioventricular re-entrant tachycardia (AVRT).
Causes and Risk Factors
The exact cause of WPW is often unknown. Most cases are related to abnormal development of the heart’s electrical conduction system before birth. Many patients have structurally normal hearts, but WPW may also be associated with congenital heart disease or inherited conditions in selected cases.
Congenital origin: the accessory pathway is usually present from birth.
Sporadic occurrence: most cases occur without a family history.
Genetic factors: rare familial cases may be linked with inherited mutations, including PRKAG2-related disease.
Autosomal dominant inheritance: in some families, the condition may pass from parent to child.
Congenital heart disease: WPW is associated with some structural abnormalities, especially Ebstein anomaly.
Cardiomyopathy: selected inherited heart muscle disorders may be associated with pre-excitation.
Clinical Manifestations
Symptoms vary widely. Some people remain asymptomatic, while others experience recurrent episodes of tachyarrhythmia. Patients may describe the heart as racing, pounding, fluttering, or beating irregularly.
Palpitations or sudden rapid heartbeat
Chest discomfort
Dizziness or lightheadedness
Shortness of breath
Fatigue
Anxiety during episodes
Syncope or near-syncope
Why Symptoms Occur
Dizziness and fainting may occur when a very rapid rhythm reduces effective cardiac output and decreases blood flow to the brain.
Chest discomfort and breathlessness may occur because a fast heart rate increases myocardial oxygen demand and reduces pumping efficiency.
Electrocardiographic Findings
A 12-lead ECG is central to diagnosing WPW. Classic ECG findings include a short PR interval, a delta wave, and a widened QRS complex. During symptomatic episodes, tachyarrhythmias may also be captured.
Short PR interval: the impulse reaches the ventricles earlier than normal because it bypasses the AV nodal delay.
Delta wave: a slurred upstroke at the beginning of the QRS complex, representing ventricular pre-excitation.
Wide QRS complex: part of the ventricle is activated abnormally before normal ventricular depolarization is completed.
Tachyarrhythmia episodes: rapid rhythms may be documented during symptoms.
Types of Arrhythmias in WPW
Orthodromic AVRT: the most common type. The impulse travels down the AV node into the ventricles and returns up the accessory pathway. The QRS complex is usually narrow.
Antidromic AVRT: the impulse travels down the accessory pathway into the ventricles and returns up the AV node. The QRS complex is usually wide.
Atrial fibrillation with WPW: a more dangerous rhythm. Chaotic atrial impulses may conduct rapidly through the accessory pathway, causing an extremely fast ventricular rate. Rarely, this can progress to ventricular fibrillation and sudden cardiac death.
Diagnostic Evaluation
Diagnosis is based on clinical history, ECG findings, and additional testing when needed. The choice of investigation depends on symptom frequency, risk level, and the patient’s overall clinical status.
Electrocardiography: a 12-lead ECG may show short PR interval, delta wave, and widened QRS complex.
Holter monitoring: records heart rhythm for 24 to 48 hours and is useful when symptoms occur frequently.
Event recorder: useful when symptoms occur occasionally and are not captured on a routine ECG.
Exercise stress testing: may help assess whether pre-excitation disappears at higher heart rates, which can suggest a lower-risk pathway.
Echocardiography: evaluates heart structure and function and screens for associated congenital or structural abnormalities.
Electrophysiological study: maps the heart’s electrical pathways, identifies the location and risk characteristics of the accessory pathway, and may be followed by catheter ablation.
Management
Management depends on symptoms, arrhythmia type, episode frequency and severity, pathway risk, patient age and occupation, and the presence of structural heart disease. Treatment decisions should be guided by ECG interpretation and cardiology or electrophysiology advice.
Acute Management During Tachycardia
If the patient is stable, management may include monitoring, vagal maneuvers, and selected medications based on the rhythm. Vagal maneuvers stimulate the vagus nerve and may slow conduction through the AV node. Examples include the Valsalva maneuver, coughing, and cold-water facial immersion in selected settings.
Medication choice must be guided by the ECG rhythm. Some drugs used for other supraventricular tachycardias may be unsafe in pre-excited atrial fibrillation because they can increase conduction through the accessory pathway.
If the patient is unstable, with features such as hypotension, collapse, severe chest pain, severe breathlessness, or altered consciousness, urgent synchronized electrical cardioversion may be required.
Definitive Treatment
For symptomatic WPW, catheter ablation is often the definitive treatment. During the procedure, a catheter is inserted through a blood vessel and guided into the heart. The accessory pathway is mapped and then destroyed using radiofrequency energy or cryotherapy. Catheter ablation is highly effective and can cure many patients.
Complications
Although many people with WPW do well, clinically important complications can occur, especially when rapid arrhythmias are recurrent or when atrial fibrillation conducts quickly through the accessory pathway.
Recurrent tachycardia
Syncope or near-syncope
Reduced quality of life due to palpitations
Atrial fibrillation with rapid ventricular response
Rarely, ventricular fibrillation
Rarely, sudden cardiac death
Nursing Considerations and Patient Education
Nursing care focuses on early recognition of symptoms, rhythm monitoring, patient safety, timely escalation, and clear education. Patients should be encouraged to seek medical care if symptoms are severe, prolonged, or associated with warning signs.
Teach patients to recognize palpitations, sudden rapid heartbeat, dizziness, syncope, chest pain, and severe breathlessness.
Advise urgent evaluation for fainting, severe chest pain, severe shortness of breath, collapse, or prolonged rapid heartbeat.
Encourage regular cardiology follow-up, especially for symptomatic patients or those with high-risk features.
Discuss avoidance of personal triggers such as excessive caffeine or stimulants when these clearly provoke symptoms.
Reinforce that symptomatic patients may benefit from electrophysiology assessment and catheter ablation.
Encourage patients not to self-medicate for palpitations without medical advice.
Prognosis
The prognosis is generally good, especially in people without structural heart disease. Many asymptomatic individuals may never develop serious problems, but risk assessment remains important. Symptomatic patients often improve significantly after successful catheter ablation.
Conclusion
Wolff-Parkinson-White syndrome is a congenital cardiac conduction disorder caused by an abnormal accessory pathway between the atria and ventricles. This pathway bypasses the normal AV nodal delay and causes ventricular pre-excitation. The condition may be asymptomatic or may cause recurrent tachyarrhythmias, especially atrioventricular re-entrant tachycardia.
Diagnosis is mainly based on ECG findings such as a short PR interval, delta wave, and widened QRS complex. Management depends on symptoms and risk level. Acute episodes may require vagal maneuvers, rhythm-specific medication, or cardioversion, while catheter ablation is the definitive treatment for many symptomatic patients. Early diagnosis, patient education, and appropriate specialist management usually lead to excellent outcomes.
Written by Vaanila Swarnamyuran
Registered Nurse
MSc Medical Surgical Nursing
TNNMC No. 205047
References
Journals
- 1.Wolff-Parkinson-White syndrome: Diagnostic and management strategiesMasihullah Barat, MD, David Torres Barba, MD, PhD and Gordon Ho, MDCleveland Clinic Journal of Medicine
Web Links
- 1.Wolff-Parkinson-White syndromeNHS - United Kingdom
Related Articles

Cerebrovascular Accident (Stroke): Causes, Symptoms, Diagnosis, Treatment, Prevention, and Rehabilitation.
Learn More

